Defeating the Trump war on women
By Malcolm Potts, MB, BChir, PhD, FRCOG.
June, 2017
Although few understood it at the time, one of the most consequential events of the past 100 years occurred in 1957. It was the first sale of an oral contraception. Today, 80% of American women are now using, or have used, oral contraceptives. For good reason, we call it “The Pill”.
The Pill has given tens of millions of women the autonomy that is their birthright. It helps young women complete their education and develop their careers. The Pill is a major factor reducing the abortion rate. But the revolution the Pill triggered is unfinished: women cannot access oral contraceptives without a physician's prescription.
The Trump presidency has launched a veritable war on women, destroying Obama care and defunding Planned Parenthood. Suddenly, countless poor and vulnerable women have no insurance and therefore no access to the Pill.
The good news is that the Bay Area is the epicenter of efforts to switch the Pill from prescription to over-the-counter (OTC) sale. The Packard Foundation has given a $12 million grant to support this work. Professor Grossman from UCSF has been the premier researcher on women's attitudes and knowledge. His work was quoted by the American College of Obstetricians and Gynecologists when they endorsed OTC sale of the Pill.
 Margaret Sanger
Margaret Sanger
Two companies are working with the FDA to demonstrate that, given appropriate labeling, women will be able to use oral contraceptives safely when sold over-the-counter. My company Cadence Health is working with what are called combined oral contraceptives and a French company HRA is working with progestin-only pills
The Pill dissolved the shackles of reproductive slavery which women had been subject to for so many generations. If that sounds a hyperbole, consider this. In 1921 an Austrian physician, Ludwig Haberlant, understood that the hormones released during pregnancy and breast-feeding could, in his words, “prove an ideal method for practical medicine and its future task of birth control.” Haberlant was criticized with such vitriol by his fellow physicians that he committed suicide.
 Ludwig Haberlant
Ludwig Haberlant
The first Pill, Enovid, whose diamond jubilee we celebrate today, was developed by two maverick scientists in a laboratory outside Boston Massachusetts shoehorned into what had been a private house. Work on the Pill would never have taken place if not for the efforts of Margaret Sanger to persuade Kate MacCormick, the inheritor of the International Harvester fortune, to support the initial research. At the time the NIH was forbidden to have anything to do with contraception. The use of any form of contraception was illegal in Massachusetts. Enovid was approved by the FDA to treat “menstrual irregularities”, although news that it also prevented conception spread like wild fire. Enovid was approved as an oral contraceptive three years later. Soon millions of women in the US and around the world were using the Pill.
In my own marriage, we switched from a messy, uncertain diaphragm to a daily pill. At that time, I was a young obstetrician and a fellow of the Cambridge college engaged in research into mammalian reproduction.
 Goody (Gregory) Pincus
Goody (Gregory) Pincus
I met Goody (Gregory) Pincus, the scientist who drove the development of the Pill, at research meetings. I asked him why did he design a pack which subjected women to unnecessary uterine bleeding every month if the Pill was intended to imitate the natural suppression of ovulation during pregnancy and breastfeeding. He agreed continuous use would be better, but felt the idea of an oral contraceptive was so radical that to also abolish monthly bleeding would be unacceptable. In the 1980s, with colleagues in Scotland I tested what we called a “tricycle pill” where women had only 4 periods a year. Half the women said, “Why didn't you invent this earlier?” Sadly, big manufacturers of the Pill, who have never been strong in innovation, refused to build on our success.
While in Cambridge in the 1960s, I helped found a clinic willing to prescribe the Pill to unmarried couples – a revolutionary thing to do at the time. Recently, at a party in San Francisco for Oxbridge alumni, a woman came up and said, “Dr. Potts you changed my life.” I didn't change her life, but the Pill I prescribed did. An unintended pregnancy in the 1960s would have destroyed her life and that of her fianc�.
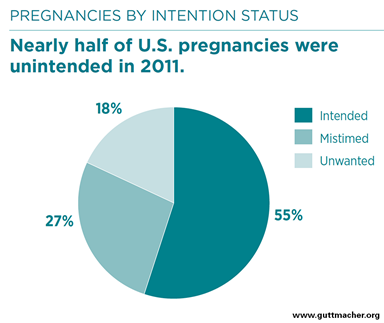
Sixty years later in America, as the Trump war on women deprives individuals of access to oral contraceptive prescriptions, taking the Pill off the prescription only list, is the only way we have of preventing women having their lives destroyed because of unintended pregnancies. Surveys show that 2.9 million women aged 15 to 44 are at risk of unintended pregnancy and this number is certain to rise as women loose medical insurance. If, when the Pill comes off prescription, a quarter of women start using the Pill, over half a million unintended pregnancies will be avoided annually, and Trump's war on women will be rolled back.

The early formulations I prescribed in the 1960s involved high doses of hormones. Sometimes there were serious side effects, including blood clots which could pass to the lungs and prove lethal. Senior researchers were convinced the Pill would cause cancer. In 1969 Barbara Seaman wrote The Doctor's Case Against the Pill, triggering hearings in congress which almost had the Pill taken off the market.
The Pill was the first medication in history to be used for several years by healthy individuals. We had entered uncharted territory. Scientifically there was no way to be certain about all the risks and benefits of using the Pill until it had been used for generations, although early studies did demonstrate that the greatest risk of venous thrombosis was in women over age 35 who smoked, and that the lowest possible dose of estrogen was also the safest.
Today, the Pill has become one of the best studied drugs in history. I remember in 1968 when the British Medical Research Council began to recruit 23,000 women using the Pill and a similar number not using it. These women have now been followed for 39 years. Women using the Pill lived slightly longer than those not using it. Pill users saw a significant decrease in cancer of the uterus, ovary and bowel and in melanomas. Although Pill users had higher rate of death from heart disease while taking the pill, over their life-time they had a lower risk of death from cardio-vascular disease.

These results encourage us to look at human reproduction in a totally new perspective. For most of human history we lived in hunter-gatherer societies where the mean age of puberty was about 19, women on average had 5 to 6 children, spaced by long intervals of breast-feeding. Because of this behavior, women may have had as few as 50 menstrual cycles in a lifetime. Today, with the early onset of puberty, smaller families, and limited breastfeeding modern women can have as many as 300 to 400 menses.
This profound change has been associated with a stunning 10 to 200-fold increase in breast, ovarian, and uterine cancer. The Pill, by imitating the hormone patterns of pregnancy and breastfeeding, partially returns women to a more natural pattern of reproduction. Pill use neither reduces nor increases breast cancer, but there is an approximately 50% reduction in ovarian and uterine cancer. About a million women, including 30% of adolescents using the Pill, choose it not for family planning but for its non-contraceptive benefits, such as lighter, less painful, and more regular periods.

In the battle to defeat Trump, it is imperative that women are given the choice of OTC sale of both the combined and progestin-only formulations. Progestin-only pills work primarily by making cervical mucus hostile to ascending sperm. Only two percent of women using the Pill choose these formulations, probably because they do not suppress ovulation consistently giving irregular periods and taking away, the non-contraceptive benefits of combined pills. Progestin-only pills must be taken close to the same time each day or the failure-rate rises, and 10% of those failures occur as ectopic pregnancies.

When Pincus began developing the Pill he started with a progestin-only formulation. However, he found that formulations, which had been accidentally contaminated with a smidgen of estrogen, worked much better. Nevertheless, the big advantage of progestin-only pills, and the reason why experts think they could be used more widely, is that they do not contain estrogen - the hormone associated with clotting problems found with combined oral contraceptives.
If the half million unintended pregnancies mentioned above are to be prevented, then both the combined and progestin-only pills have essential roles. However, in my opinion, there is no doubt that the combined pill, will be the most effective method of birth control.
Dr Potts is an emeritus professor in the School of Public Health, University California, Berkeley and founding chairman of Cadence Health, which has the mission of selling the Pill over the counter.